

Obesity is the most prevalent lifestyle-related health condition in the United States. The rates of obesity have tripled since the 1970s, culminating in 36% of the adult population categorized as obese and 69% as overweight.1,2
The development of obesity is a multi-factorial and individualized process. Both genetics and environmental conditions contribute to the development of excessive adiposity. Weight loss solutions are necessary for optimal health because many obesity comorbidities increase mortality risks.3
Hunger vs. Satiety Signals in Obesity
For those with obesity, there is often a dysregulation of hunger and satiety signals that can make weight loss difficult. The below chart provides examples of the hunger and satiety signals that can become dysregulated.
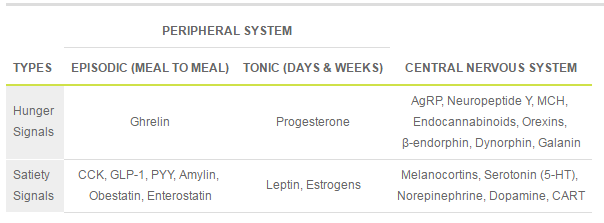
Image Source: Body Weight, Appetite and Lipocalin. Creative Biomart Blog. Published April 8, 2017.
Some hunger and satiety hormones are better known than others. Episodic satiety signals like cholecystokinin (CCK), peptide YY (PYY) and glucagon-like peptide-1 (GLP-1) can have decreased activity in those with obesity, leading to increased hunger signals. Ghrelin, an episodic hunger hormone, is normally suppressed with food intake; however, that suppression is often impaired in those with obesity. Resistance to leptin signaling is a well-understood mechanism of impaired satiety signaling in those with obesity. Lastly, impaired serotonin or dopamine signaling can cause overeating.4
Semaglutide: A Novel Weight-Loss Drug
Targeting satiety signaling in the body is the mechanism of action for most pharmaceuticals approved for treating obesity.1 Semaglutide has exploded in popularity as a treatment for obesity ever since the FDA approved the branded drug Wegovy® on June 4, 2021.4 Semaglutide is the generic form of the GLP-1 receptor agonist drug class originally developed for diabetes treatment.
GLP-1 is a gut-derived incretin hormone released in response to food intake to signal satiety.4,6 There are several mechanisms by which GLP-1 promotes satiety:
- Stimulates insulin secretion from the pancreas in the presence of glucose
- Inhibits glucagon secretion
- Slows gastric emptying7
- Receptors present in various locations of the brain related to satiety, reward and motivation (food cravings)1,4
Semaglutide is a structurally altered analog of endogenous GLP-1 that extends its half-life in the body to 160 hours, making it adequate for once-weekly administration.7 The prolonged action of the medication leads to an overall decrease in calorie intake, resulting in weight loss.
A series of clinical trials called the STEP (Semaglutide Treatment Effect in People with obesity) program was developed to assess the efficacy and safety of semaglutide for obesity treatment. The weight loss benefits of semaglutide were proven over placebo in all the studies. Semaglutide also shows greater efficacy than other approved pharmaceutical drugs for weight loss. The average weight loss found in the trials with once-weekly semaglutide injection was an astounding 14.9-17.4% of original body weight. For comparison, behavioral intervention in diet or exercise alone usually only results in 5-10% body weight loss.8
Semaglutide Limitations and Challenges
Many medications have side effects that can cause uncomfortable symptoms. The frequency of reported adverse events with semaglutide is between 81.3-95.8% of users.7 The most frequently reported side effects are gastrointestinal symptoms, including nausea, vomiting, constipation and diarrhea, that are usually transient and mild to moderate in severity. Discontinuation of semaglutide treatment in clinical trials due to side effects occurred at a rate of 4.9-12% of participants.1,6 Other side effects less frequently reported include the following:
- Hypoglycemia
- Cholelithiasis6
- Cholecystitis4
- Pancreatitis
- Acute kidney injury6
- Urinary tract infections
- Nasopharyngitis
- Upper respiratory tract infections
- Dizziness
- Headache4
- Diabetic retinopathy8
- Thyroid cancer9
- Injection site reactions6
Semaglutide is not safe for use in all people. It is not recommended for those with type 1 diabetes or a history of ketoacidosis. It should not be used in those with a personal or family history of medullary thyroid cancer or multiple endocrine neoplasia type 2 (MEN2). Semaglutide cannot be used in those who are currently pregnant or breastfeeding. Significant caution and a risk-versus-benefit assessment should be performed for those with a history of gallbladder disease, pancreatitis or diabetic retinopathy.9
The cost of semaglutide is another factor that may hinder its use for some. Currently, Wegovy® is the only FDA-approved—meaning possibly covered by insurance—form of semaglutide for weight loss. Generic semaglutide, Ozempic® and Rybelsus® can be used off-label for weight loss, but those come at a high monthly cost that can be difficult for people to afford long term.
Avoiding Weight Regain After Stopping Semaglutide
Patients discontinuing pharmaceutical weight loss medication need additional support to minimize the risk of weight regain. In the STEP 4 trial, after 20 weeks of semaglutide, the intervention group was randomized to either continue with semaglutide or switch to a placebo. The group that was kept on semaglutide continued to lose weight, whereas the group that was placed on a placebo regained an average of 6 kg (13.2 lb) of weight that was lost.6
Weight regain occurs because the body has a drop in metabolism from the lost adipose tissue and an increase in hunger signaling as the body attempts to regain the lost energy reserves. This process is called the “energy gap,” and it is a significant factor in why long-term weight management often fails.10
How Polyphenols Can Bridge the Energy Gap
A blog post from earlier this year titled “Promising New Weight Loss Research: Can Specialized Polyphenols Provide the Spark Your Patients Need?” detailed how certain plant extracts high in polyphenols can help to bridge the energy gap. A combination of Hibiscus sabdariffa, lemon verbena extract and decaffeinated green coffee bean extract have been found to increase endogenous satiety hormones like GLP-1 to control hunger and manage cravings. These plant extracts are a novel way to minimize weight regain after withdrawing from weight loss medication like semaglutide.
The Bottom Line
To date, semaglutide has been shown to be the most efficacious pharmaceutical intervention for weight loss support. It can be a great tool to initiate weight loss, especially in those with chronic obesity, obesity-related comorbidities or for those who experience difficulty losing weight with diet and exercise. The cost of treatment makes semaglutide unrealistic for most people to continue taking it long term. In that case, they need other behavioral and nutritional support like plant polyphenols to make their weight loss journey a continuing success.

Megan Borreson, ND is the CM Vitals Clinical Brand Manager at Lifestyle Matrix Resource Center. She attended undergraduate school at the University of Wisconsin–Eau Claire and received her Bachelor of Science degree in cell biology and a Bachelor of Arts degree in Spanish with a minor in chemistry. Dr. Borreson then enrolled at National University of Health Sciences where she graduated summa cum laude with a Master of Acupuncture and Doctorate of Naturopathic Medicine.
References
- Singh G, Krauthamer M, Bjalme-Evans M. Wegovy® (semaglutide): a new weight loss drug for chronic weight management. J Investig Med. 2022;70(1):5-13. doi:10.1136/jim-2021-001952
- Adult Obesity. Obesity Prevention Source. Harvard T.H. Chan School of Public Health. Published October 21, 2012. https://www.hsph.harvard.edu/obesity-prevention-source/obesity-trends-original/obesity-rates-worldwide/
- Apovian CM. Obesity: definition, comorbidities, causes, and burden. Am J Manag Care. 2016;22(7 Suppl):s176-s185.
- Mahapatra MK, Karuppasamy M, Sahoo BM. Therapeutic Potential of Semaglutide, a Newer GLP-1 Receptor Agonist, in Abating Obesity, Non-Alcoholic Steatohepatitis and Neurodegenerative diseases: A Narrative Review. Pharm Res. 2022;39(6):1233-1248. doi:10.1007/s11095-022-03302-1
- Body Weight, Appetite and Lipocalin. Creative Biomart Blog. Published April 8, 2017. Available at: https://www.creativebiomart.net/blog/body-weight-appetite-and-lipocalin/
- Smits MM, Van Raalte DH. Safety of Semaglutide [published correction appears in Front Endocrinol (Lausanne). 2021 Nov 10;12:786732]. Front Endocrinol (Lausanne). 2021;12:645563. Published 2021 Jul 7. doi:10.3389/fendo.2021.645563
- Deng Y, Park A, Zhu L, Xie W, Pan CQ. Effect of semaglutide and liraglutide in individuals with obesity or overweight without diabetes: a systematic review. Ther Adv Chronic Dis. 2022;13:20406223221108064. Published 2022 Jul 4. doi:10.1177/20406223221108064
- Bergmann NC, Davies MJ, Lingvay I, Knop FK. Semaglutide for the treatment of overweight and obesity: A review. Diabetes Obes Metab. 2023;25(1):18-35. doi:10.1111/dom.14863
- Common Side Effects of Wegovy® (no date) Wegovy®. Available at: https://www.wegovy.com/taking-wegovy/side-effects.html (Accessed: 27 July 2023).
- Boix-Castejón M , Herranz-López M , Pérez Gago A , et al. Hibiscus and lemon verbena polyphenols modulate appetite-related biomarkers in overweight subjects: a randomized controlled trial [published correction appears in Food Funct. 2018 Jul 17;9(7):4037]. Food Funct. 2018;9(6):3173-3184. doi:10.1039/c8fo00367j

